
Author: Dom Fransen, 2024
The global rise in mental health concerns indicates an increasing need for effective healing modalities to help people work through mental health disorders. Given the powerful history of certain psychoactive substances, MDMA is being carefully trialed alongside therapy in the treatment of various mental health disorders including Post Traumatic Stress Disorder (PTSD). In fact, the Therapeutic Goods Administration (TGA) in Australia has approved the use of certain psychedelic medicines for therapeutic use. As of July 1st, 2023, authorized psychiatrists can prescribe the psychedelic substance MDMA for the treatment of post-traumatic stress disorder (PTSD) provided professional therapy serves alongside the drugs administration. There is momentum within the scope of this clinical treatment as western medicine discovers the potential of psychedelics in combination with therapy to help remedy certain mental health disorders.
In MDMA studies the therapeutic techniques and processes have been integral for translating potential insights from the trial space into real word practice. The therapeutic effect is not simply due to the physiological effects of the substance ingested, rather successful MDMA-assisted psychotherapy treatment for PTSD hinges on the careful combination of therapeutic set and setting, and the interactions between patient and psychotherapist(s) throughout each stage of the process. This raises important questions about whether psychotherapy is the most effective method for the job, its impact on outcomes, and ultimately how psychotherapy can ensure optimal treatment benefits are achieved whilst prioritizing patient safety in the psychedelic medicine space. This evaluative review describes the history and effects of MDMA on humans, why psychotherapy is the most applicable therapy, the process of MDMA-assisted psychotherapy and its remarkable results in treating PTSD symptoms, and lastly suggestions for future research and development in the field of psychedelic-assisted therapy. Research illuminates the remarkable impact of psychedelic-assisted psychotherapy in the treatment of PTSD. As these studies shift from clinical trials to approved therapeutic practices, prioritization of well-established infrastructure is essential to stimulate growth, understanding, and application within the psychedelic-assisted therapeutic field.
MDMA: History and Effects on humans
Sourced from: Cuthbertson, C R. (2023)
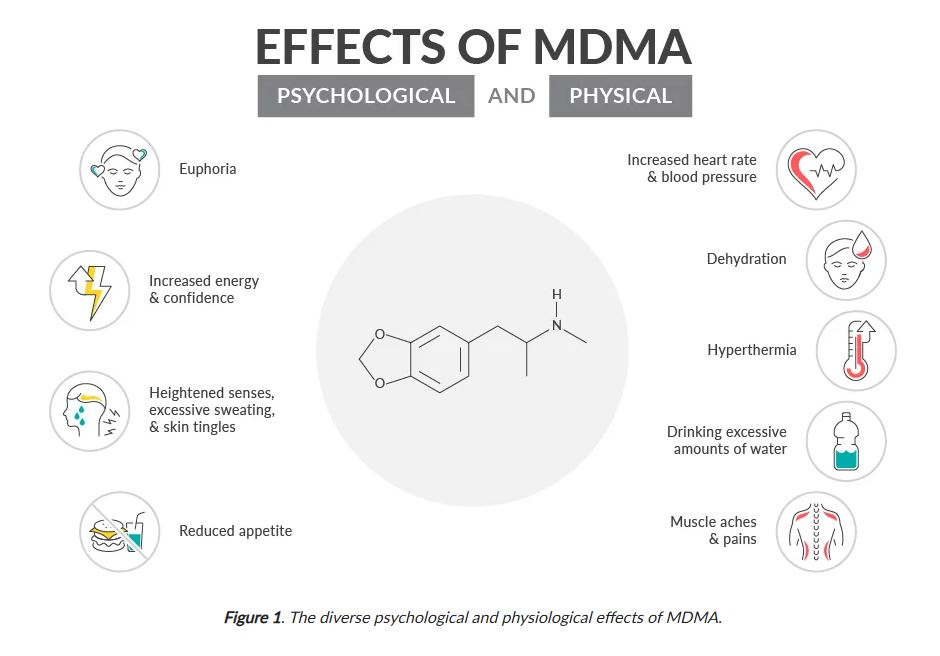
MDMA (3,4- Methylenedioxymethamphetamine) is a powerful psychoactive amphetamine that causes elevated mood, increased energy, and feelings of bonding among other effects (see figure 1), and is categorized as an entactogen. In 1912, MDMA was first synthesized by the Merck scientist Dr. Anton Köllisch, his research of MDMA continued into the late 1920s, but for economical reasons the research was cut short. Not until decades later was the psychotropic activity of MDMA mentioned in mainstream research (see Table 1)1. We can see from the table timeline below that from 1943 great progress was made in psychedelic research to more controlled medical use, in fact psychologists and psychiatrists in the 1950s noted that they may “…serve as new tools for shortening psychotherapy”2. That is until 1970 which saw the control substances act firmly restricting clinical use of psychotropic substances and thus halted further research for decades.
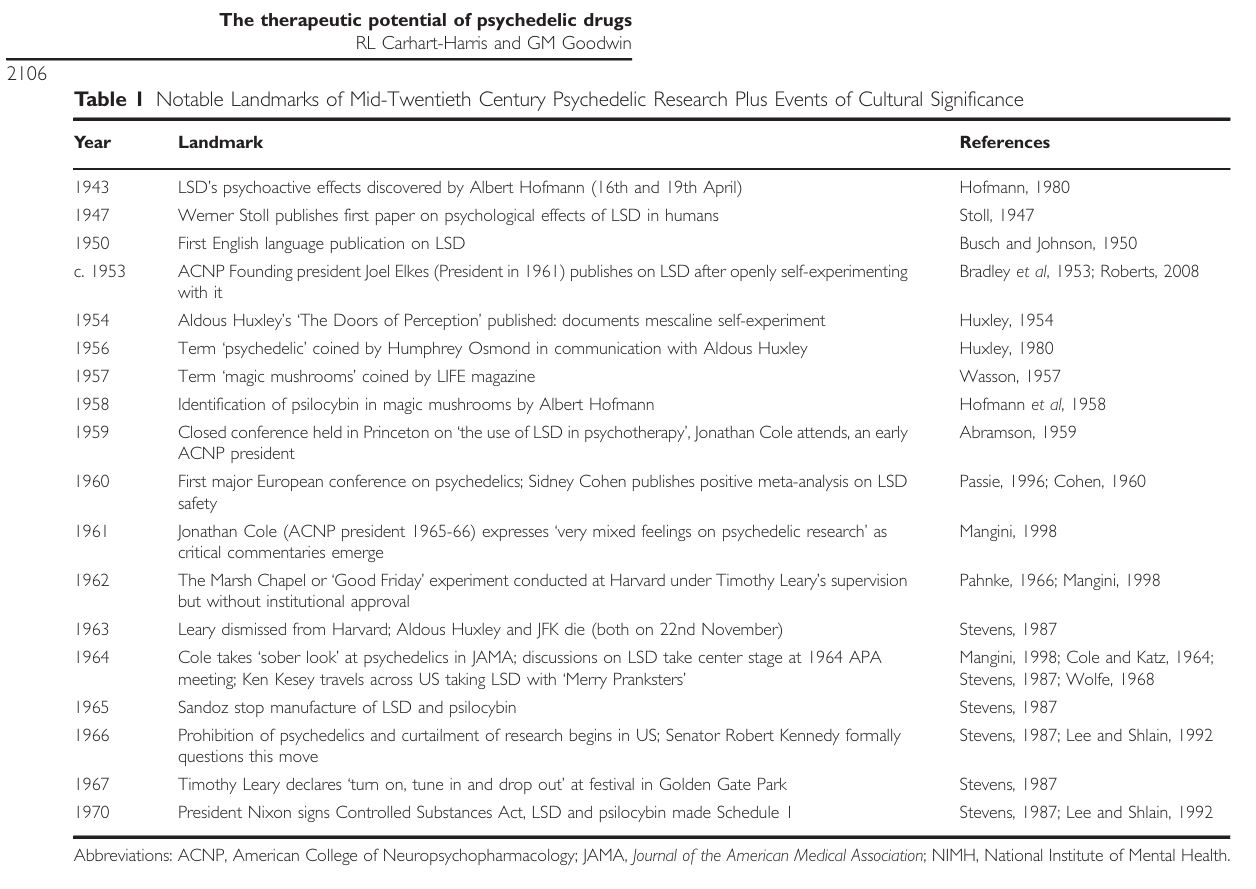
Table 1: Sourced from – Carhart-Harris, R. L., & Goodwin, G. M. (2017). The therapeutic potential of psychedelic drugs: past, present, and future. Neuropsychopharmacology, 42(11), 2105-2113.
Why Psychotherapy?
Indeed, psychedelics have been used by many cultures, for various purposes, and in different contexts ranging from indigenous holistic healing and sacrament, to carefully controlled clinical trials using specific psychedelics. Psychedelic research has been primarily focused on the acute psychedelic experience being the major catalyst to positive change. As a result, research falls short in fully recognizing the role of other key components like set and setting (environment), sensory stimuli or lack of (music and fragrances), and the psychotherapy working alongside the psychedelic. The most salient factor connecting successful ancient healing experiences to modern clinical trials is the presence of a guide, healer, shaman, or therapist that can support the person having the psychedelic experience. Of course, people are aware of psychedelic experiences described as a ‘bad trip’, although it is less common with MDMA, when there is minimal or no guidance with powerful chemicals such as LSD, Psilocybin, and many plant psychedelics some people can get confused or lost resulting in a bad psychoactive experience that fails to resolve in the intended way. This is precisely why having an effective therapy operating alongside the medication is fundamental.
With that in mind, psychedelic-assisted psychotherapy is a mental health intervention involving the administration of psychoactive substances with the support of a professional psychotherapist3. There are copious reasons for the preferability of psychotherapy in psychedelic research, such as integration of psychedelic experiences, safety and emotional Support, enhanced therapeutic outcomes, guided exploration, personalization of treatment, focus on long-term change, and mitigation of risks. In other words, PAP provides a structured, supportive framework that helps patients to better integrate intense and challenging experiences as opposed to medication-only, physical, or alternative healing modalities.
MDMA-assisted psychotherapy
MDMA-assisted psychotherapy has produced remarkably positive outcomes for reducing PTSD symptoms through rigorous consideration of therapeutic dosage, the key effects MDMA elicits, the importance of set and setting, and the psychotherapeutic process. Firstly, the therapeutic dose administered to patients within a typical clinical MDMA session is 125 mg, which is said to last approximately 4-8 hours4. Secondly, MDMA elicits a variety of subjective effects including increased feelings of connection, empathy, and interpersonal trust (figure 1) which appears to encourage the patients’ ability to respond to the treatment in a beneficial way. Put simply, MDMA, a type of amphetamine, increases the release of certain brain chemicals and hormones that may help regulate brain circuits involved in processing traumatic memories4. Third, there is a special emphasis on safety when it comes to set and setting which has resulted from various negative occurrences and mishaps under the influence of psychedelic substances. For the most beneficial outcomes ideally two responsible co-therapists are present in the room administering the substance, the patient is blindfolded to avoid external visual stimuli, and the room itself is prepared to be comfortable and pleasant for the duration of the session so patients are not at risk of hurting themselves or others during the experience. Lastly, the psychedelic-assisted psychotherapeutic process is imperative for positive therapeutic outcomes, working as a standardized scaffolding system that supports patients through often intense and vulnerable sessions incorporated within modern studies.
To further conceptualize the function of MDMA-assisted psychotherapy, it is typical that psychedelic-assisted therapy is broken up into three stages of therapeutic sessions, they are: the preparatory, medication, integration sessions5. In brief, the preparatory session(s) is where the therapist and/or co-therapist encourages the patient to explore the history of his/her life, placing the emphasis on the patient’s understanding of their symptoms, intentions, expectations, and the potential for emotional and psychological growth. This crucial phase of the treatment process is where the therapeutic alliance begins to form. Prior to the ingestion of any psychedelic medicine a relationship is formed which ensures the container in which the medicines are taken feels as familiar and supportive as possible. Secondly, the medication sessions involve the patient’s ingestion of the psychedelic drug within a comfortable and appropriate set and setting accompanied by a male and female co-therapy team. During this session, with the guidance of the co-therapists the patient takes an inward focus with the assistance of music and an eye mask, with a 6-8-hour window for the therapists to empathetically listen to the patient in a neutral and non-threatening way. Most importantly, the integration sessions are for the therapists to translate the patient’s psychedelic experience into meaningful long-term change by highlighting insights, thoughts, and ideas that are illuminated within their psychedelic session5.
MDMA-assisted psychotherapy for treatment of PTSD
MDMA- assisted psychotherapy has been under thorough investigation in the clinical world ever since the twentieth century with remarkable results for its effectiveness in reducing PTSD symptoms. For example, an analysis of six randomized double-blind clinical trials revealed that patients were experiencing significantly greater reductions in PTSD symptoms with the use of MDMA- assisted psychotherapy, which was measured within clinically appropriate conditions using the DSM-IV PTSD scale4. Additionally, MAPS’ (Multidisciplinary Association for Psychedelic Studies) research on MDMA and PTSD has provided strong evidence for the effectiveness of MDMA in therapeutic settings. One of their earliest experimental research studies concluded that “MDMA-assisted therapy can be administered to PTSD patients without evidence of harm”6. Additional evidence from the MAPS (Multidisciplinary Association of Psychedelic Studies) compared MDMA-assisted psychotherapy and manualized therapy with inactive placebo7. This showcased that over the course of three MDMA-assisted psychotherapy sessions PTSD symptoms and functional impairment were significantly reduced in comparison to the placebo group, which suggests that the combination of both the psychoactive substance and therapy produces the greatest treatment benefit.
Future Research
Despite the promise of this new treatment modality there are several limitations that should be considered. Firstly, psychotherapy has been the main therapeutic method employed however there is evidence to suggest other methods may also be efficacious. For example, in one study participants received MDMA and Cognitive Behavioral Conjoint Therapy (CBCT) and significant improvements in PTSD symptoms were observed8. This suggests that positive outcomes may not be limited to psychotherapeutic models, and that other therapeutic techniques should be explored. A further consideration as discussed is that the successful translation of psychedelic-assisted psychotherapy into clinical practice will rely on several factors including adequate expertise, procedures, and ethical standards9. One-way therapeutic psychedelic researchers have looked to overcome this concern is to integrate more holistic mindfulness-based models such as ACE (Acceptance, commitment, Embodiment) which adopt key principles from ACT therapy and merge these into the structured process of psychedelic-assisted therapy.
Other recommendations from those within the field include the establishment of a multidisciplinary committee for psychedelic therapies involving research, clinical, regulatory, industry, and community interests9. This is an interesting point to consider as more countries like New Zealand are now realizing the therapeutic potential of PAP for these disorders. Australia and New Zealand have the facilities, however, requires governmental, academic, and public acceptance of psychedelic therapy as an effective tool in treatment of various deep-set disorders in their populations10. To maximize the potential benefits of these treatments a well-established infrastructure transcending across these sectors needs to be a priority. Future research should carefully consider the therapist training, alongside the characteristics of both the therapist and the participants to enable a stronger therapeutic alliance, while also taking in account therapist’s adaptability, that is shifting from styles that may hinder therapeutic alliance11. Finally, to ensure the safety efficacy and sustainability of these treatments, training and accreditation of psychedelic therapists should be prioritized and a comprehensive training program developed9. Ultimately, consideration of these points will allow for a more cohesive and supportive infrastructure in which these psychedelic-assisted therapies may develop.
Conclusion
Overall, studies incorporating psychedelic-assisted psychotherapy for the treatment of PTSD have generated remarkably positive results. However, when psychotherapy is not incorporated in treatment the results are nowhere near as promising. Taking into consideration how these psychedelics were used in various cultural traditions and throughout previous psychedelic research, there is a clear emphasis on the importance of a guide, shaman, or therapist that assists and supports the person or patient having the psychedelic experience. Necessarily, researchers have done numerous studies of MDMA-assisted psychotherapy through privately funded NGO’s such as MAPS where the combination of professional psychotherapy marked significant reductions in PTSD symptoms. These studies provided significant psychological evidence that has effectively contributed to the approval of psychedelic-assisted therapy in some areas of the world. Psychotherapy and its complex regulatory training body must be a key consideration as these treatment modalities shift from clinical trials to psychedelic-assisted therapy clinics, with the potential to eventually evolve into supportive psychedelic-assisted community therapy centers. Finally, a well-established infrastructure involving research, clinical, regulator, industry and community needs to be prioritized to stimulate further growth, understanding, and applications within the psychedelic-assisted therapeutic field. Future research should explore other therapeutic methods and approaches that may have great potential within the psychedelic-assisted therapy space. Potentially combining and adopting approaches from CBT and ACT could form promising approaches to further reduce symptoms in PTSD with the potential to be effective for many more disorders.
References:
4 Bird, C. I. V., Modlin, N. L., & Rucker, J. J. H. (2021). Psilocybin and MDMA for the treatment of trauma-related psychopathology. International Review of Psychiatry, 33(3), 229–249. https://doi.org/10.1080/09540261.2021.1919062
2 Carhart-Harris, R. L., & Goodwin, G. M. (2017). The therapeutic potential of psychedelic drugs: past, present, and future. Neuropsychopharmacology, 42(11), 2105-2113.
11 Carhart-Harris, R., Giribaldi, B., Watts, R., Baker-Jones, M., Murphy-Beiner, A., Murphy, R., … & Nutt, D. J. (2021). Trial of psilocybin versus escitalopram for depression. New England Journal of Medicine, 384(15), 1402-1411.
1 Cuthbertson, C R. (2023) MDMA: From Rave Drug to Rave Reviews in Clinical Trials. Url: MDMA From Rave Drug to Rave Reviews in Clinical Trials | News & Announcements | Cayman Chemical.
Gukasyan, N., Davis, AK., Barrett, FS., et al. (2022). Efficacy and safety of psilocybin-assisted treatment for major depressive disorder: Prospective 12-month follow-up. Journal of Psychopharmacology. 2022;36(2):151-158. doi:10.1177/02698811211073759
10 Inserra, A. (2019). Current status of psychedelic therapy in Australia and New Zealand: Are we falling behind?. Australian & New Zealand Journal of Psychiatry, 53(3), 190-192.
Johnson, M., Richards, W., Griffiths, R. (2008). Human hallucinogen research: guidelines for safety. J Psychopharmacology 22: 603-620 (PDF)
7 Mitchell, J.M., Bogenschutz, M., Lilienstein, A. et al. (2021). MDMA-assisted therapy for severe PTSD: a randomized, double-blind, placebo-controlled phase 3 study. Nat Med 27, 1025-1033. https://doi.org/10.1038/s41591-021-01336-3
6 Mithoefer, MC., Wagner, MT., Mithoefer, AT., Jerome, L., Doblin, R. (2010). The safety and efficacy of ±3,4-methylenedioxymethamphetamine-assisted psychotherapy in subjects with chronic, treatment-resistant posttraumatic stress disorder: the first randomized controlled pilot study. Journal of Psychopharmacology. 2011;25(4):439- 452. doi:10.1177/0269881110378371
8 Monson, CM., Wagner, AC., Mithoefer, AT., Liebman, RE., Feduccia, AA., Jerome, L., Yazar- Klosinski, B., Emerson, A., Doblin, R., Mithoefer, MC. (2020). MDMA-facilitated cognitive-behavioral conjoint therapy for posttraumatic stress disorder.
3 Murphy, R., Kettner, H., Zeifman, R., Giribaldi, B., Kartner, L., Martell, J., Read, T., Murphy-Beiner, A., Baker-Jones, M., Nutt, D., Erritzoe, D., Watts, R., & Carhart-Harris, R. (2022). Therapeutic Alliance and Rapport Modulate Responses to Psilocybin Assisted Therapy for Depression. Frontiers in pharmacology, 12, 788155. https://doi.org/10.3389/fphar.2021.788155
5 Reiff, C. M., Richman, E. E., Nemeroff, C. B., Carpenter, L. L., Widge, A. S., Rodriguez, C. I., … & Work Group on Biomarkers and Novel Treatments, a Division of the American Psychiatric Association Council of Research. (2020). Psychedelics and psychedelic-assisted psychotherapy. American Journal of Psychiatry, 177(5), 391-410.
9 Williams, M. L., Korevaar, D., Harvey, R., Fitzgerald, P. B., Liknaitzky, P., O’Carroll, S., … & Bennett-Levy, J. (2021). Translating psychedelic therapies from clinical trials to community clinics: building bridges and addressing potential challenges ahead. Frontiers in Psychiatry, 12, 737738.